Surgical Negligence Claims
If you have undergone a medical procedure and have suffered harm as a result of negligence by a surgeon or another medical professional, you could be entitled to compensation. At Potter Rees Dolan, we have a team of specialist solicitors who can help you make a successful surgical negligence claim - potentially a key milestone in getting your life back on track following your traumatic experience.
Our solicitors will identify who is responsible for your injuries and help you to make a claim for compensation. We will always do this in a sensitive yet efficient manner to help you through this difficult time.
Our highly reputable clinical negligence team includes Helen Dolan, Lesley Herbertson, Gill Edwards and Helen Budge, who have more than 80 years’ combined legal experience between them. All have been featured in the prestigious Legal 500 and Chambers guides, demonstrating the high level of regard in which they are held.
For access to the best possible legal advice and expertise for your case, call Potter Rees Dolan today on 0800 027 2557, or simply fill out our online contact form at the side of the page and we will get back to you.
What are the most common reasons for surgical negligence claims?
Surgical negligence compensation can be claimed for a wide variety of surgical complications, including:
- anaesthetic awareness (waking up whilst under anaesthesia)
- organ damage
- brain damage
- nerve damage
- objects left inside patients
- infection
This list is not exhaustive, and you should contact one of our solicitors if you think that you have been the victim of surgical negligence.
How can Potter Rees Dolan help?
Potter Rees Dolan’s clinical negligence team is widely regarded as one of the best in the UK. With a combined experience in serious injury law of over 80 years and comprehensive medical insight, the team is dedicated to helping patients and their families recover the compensation they deserve.
Throughout your claim, we will provide you with the support, advice and representation you need at every stage, including during the investigation, negotiation and trial processes. Our goal is always to secure the best possible settlement for your claim.
Helen Dolan, head of our clinical negligence department, was featured in the Chambers 2020 legal guide, which said: "Helen regularly handles complex claims, such as those related to psychiatric care. She has further expertise in spinal injury, surgical negligence and cerebral palsy claims, as well as breach of duty cases. One source states: 'Her attention to detail and knowledge of the case inside and out was exemplary.’”
The same publication said Lesley Herbertson “is very good on the complex details of the case and is able to translate this to clients", while Gill Edwards was described as being "incredibly good with clients - they really warm to her - and very good on the medical details".
The Legal 500 describes both Helen Budge and Hannah Bottomley as "approachable, supportive, thorough and extremely knowledgeable. They are also happy to listen to our suggestions and together we have an excellent plan in place."
Chambers 2020 also offered praise for our entire clinical negligence team, calling it a “well-regarded team with an impressive caseload of complex clinical negligence work” and citing sources that highlight the "really nice, bespoke, high-quality" service we have to offer.
Our clients tell us that the empathy and care with which we act is what sets us apart. We specialise in serious and catastrophic injuries, so we know how difficult it can be to live with severe disability or illness. It is our aim, therefore, to make the claims process as stress-free as possible for you and your family.
Funding a surgical negligence claim
The majority of clinical negligence cases are funded on the basis of a “no win, no fee” arrangement, also known as a Conditional Fee Agreement. This means we can investigate your potential claim without you having to pay any costs if the case is not successful; the details of how this arrangement works will be explained to you during our first meeting.
If you already have a legal expense insurance policy in place, we will always start by looking into whether you can use this policy before considering whether a Conditional Fee Agreement would be more appropriate.
What happens next?
We will start by discussing your circumstances to understand whether or not you have a viable legal case. If we agree that you do, we will help you to gather the evidence required to build a strong claim that will give you the best chance of recovering the right amount of compensation.
To accomplish this, we will review all relevant medical records with you, before instructing independent experts in the appropriate disciplines to advise on whether or not you have received substandard treatment. Once the supporting evidence has been obtained, we will put the claim to the defendant and, if necessary, we will commence court proceedings and progress the claim as quickly as possible.
In appropriate cases, where liability is admitted at an early stage, we will work towards obtaining interim compensation payments to help you to put in place any support that is required with care and therapy.
Contact us today
If you believe that you may be entitled to compensation, call us today on 0800 027 2557. Alternatively, get in touch through our contact page, or speak to a specific member of our team by visiting their profile on our people page.
Useful Information
Amniotic Membrane Transplantation (AMT)
What is the amniotic membrane?
The amniotic membrane is the innermost layer of the placenta and can be used as a graft or dressing in a range of different surgical procedures, typically involving the eye. It is used for its anti-inflammatory and anti-scarring effects.
What is amniotic membrane transplantation (AMT)?
This describes the surgery performed in which the amniotic membrane is used as a graft or as a dressing.
In ophthalmology, AMT has been used in the revision of scars in the eye and also correcting defects following the removal of
Generally, the amniotic membrane is obtained through donors, who have been screened for diseases such as HIV, undergoing a caesarean section.
Surgeons clean the placenta with a mixture of salt solution, penicillin and other ingredients. The amnion is separated through sterile dissection and stored in a glycerol solution.
Bile Duct Injury
What is bile?
Bile is a fluid in the digestive system that is stored in the gall bladder, which helps to break down food and get rid of toxins from the body.
Bile ducts and the biliary system
The biliary system is made up of a series of tubes and organs, beginning with the liver and ending with the small intestine. There is also a number of bile ducts, such as the common bile duct and the hepatic duct.
Causes of bile duct injuries
Injuries to the bile duct are most common during laparoscopic gall bladder surgery, where it may be cut, pinched or burned. If the bile duct is
Symptoms
Bile duct injuries could cause the following symptoms:
- Fever
- Nausea
- Abdominal pain
- Vomiting
- Swelling
- Jaundice
- Chills
Treatment and surgery
Once the injury to the bile duct has been noted, the main goal is to manage the infection and leakage caused by the injury. The surgeon may have to reconstruct the bile duct using a piece of intestine to bypass the blockage.
Most bile duct injuries are successfully
Small bowel resection
This surgery removes part or all of your small bowel (small intestine) when it is blocked or diseased.
Most digestion (breaking down and absorbing nutrients) of the food you eat takes place in the small intestine. The surgery can be performed laparoscopically or with open surgery.
Small bowel resection is used to treat:
- A blockage in the intestine caused by scar tissue or congenital (from birth) deformities
- Bleeding, infection, or ulcers caused by inflammation of the small intestine. Conditions that may cause inflammation include regional ileitis, regional enteritis, and Crohn's disease
- Cancer
Carcinoid tumor- Meckel's diverticulum
- Noncancerous (benign) tumors
- Precancerous polyps
Most people who have a small bowel resection recover fully. Even with an
Corneal Graft/Transplant
This is an operation to remove the damaged cornea in the eye and replace with healthy tissue to improve sight or treat a severe infection.
The cornea is the clear outer layer of the
A corneal graft/transplant can be performed in a number of ways. These include: penetrating
After about one in five corneal transplants, the patient may reject the foreign body as the immune system attacks the transplanted cornea. This rejection can often be treated with a dose of steroid eye drops.
Other complications after a corneal transplant include astigmatism where the cornea is not a perfectly curved shape as it should be. The pressure could build up in the
Also,
Laminectomy
This is one of the most common back surgeries where a surgeon removes the rear portion of one or more spinal bones (vertebrae).
Ligaments and bones that are pressing on the nerves may be removed at the same time during surgery.
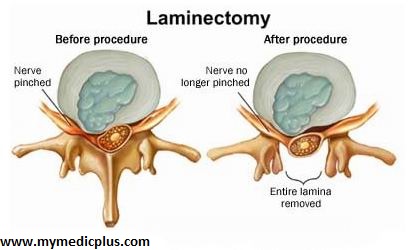
People with arthritis in their spine can sometimes develop bony overgrowths within the spinal canal which can cause the pressure.
As with any form of surgery, there can be complications during a
- Bleeding,
Infection blood clots,- Nerve injury
Most people who undergo a
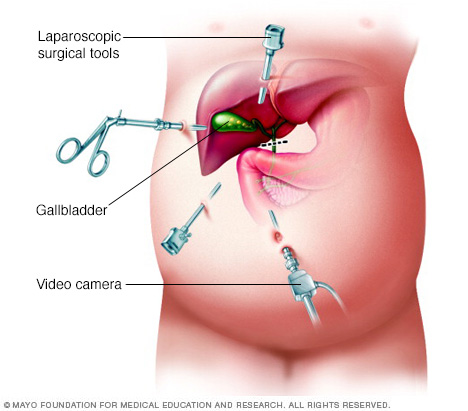
Laparoscopic Cholecystectomy
This is a surgical procedure to remove the
The use of a
There is usually also less pain with this procedure than with a normal
The removal of the gall bladder is one of the most common operations performed in the UK.
Sometimes the cholesterol, salts and waste products become out of
When the gallstones become an issue, this is when a laparoscopic cholecystectomy is usually recommended.
Gallstones can often have no symptoms and can remain undetected. However, they can become trapped in the bile duct, irritate and inflame the gallbladder or travel to other parts of the body.
Your body will still function without the gallbladder - the liver will still produce bile to digest food.
However, some people have reported bloating and
Microdiscectomy
This is a form of spinal surgery to decompress the spine using a microscope to view the spine and the lumbar disc.
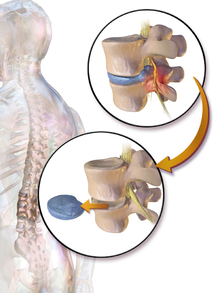
A small portion of the bone over the nerve root is removed to relieve neural impingement and to provide the nerve with more room to heal.
Compression of the spine can cause substantial leg pain and a
The success rate of a
In any spinal surgery, there is the risk of a
Salpingo-Oophorectomy
This is a surgical procedure which can be either unilateral or bilateral.
Unilateral is where the
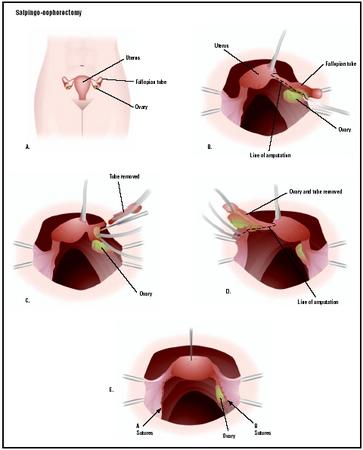
The reasons for this surgery to be performed is usually to treat forms of
This procedure may also be done to treat endometriosis as well as if a woman has been diagnosed with an ectopic pregnancy.
Salpingo-oophorectomy is considered major surgery if performed through an abdominal incision and would require three to six weeks to fully recover.
However, if the procedure if performed laparoscopically, the recovery time can be much shorter.
Immediately following the operation, sharply flexing the thighs or the knees should be avoided.
And if the patient suffers with persistent back pain or blood in the urine then it may indicate that a
Other complications, as with most major surgeries, can include infection,
Complications after a salpingo-oophorectomy, however, can include changes in sex drive, hot flashes and other menopausal symptoms if both ovaries are removed.
In general, studies have shown that the complication rate following salpingo-oophorectomy is essentially the same as that following hysterectomy.
Sarocolpopexy
This is a surgical technique used to repair a pelvic organ prolapse to restore the vagina to its normal position and function.
Reconstruction can be made using an open abdominal technique or through minimally invasive surgery such as a laparoscopy, depending on the severity of the pelvic prolapse.
A permanent synthetic mesh is used as a graft to cover the front and back surfaces of the vagina. The mesh is then attached to the tail bone and covered by a layer of tissue which lines the abdominal cavity called the peritoneum which prevents the bowel getting stuck to the mesh.
Although the majority of women fully recover from this surgery, there is a small risk that a prolapse can develop in another part of the vagina which could require further surgery.
Other complications can include; pain during intercourse, exposure of the mesh in the vagina and damage to the bladder, bowel or ureters. There are also more general risks associated with this surgery such as wound infection or a urinary tract infection.
Ureteric Implant
Some children are born with their ureters not joining the bladder in the correct place which can cause a condition called vesio-ureteric relux (VUR).
This can cause the valves to fail, allowing urine to flow backwards from the bladder to the kidneys, which can cause kidney failure.
The ureteric implant operation involves disconnecting the ureters and re-attaching them to the bladder in the correct place.
The end of the urecters joining the bladder are surrounded by muscle to strengthen the valves to reduce the chance of backwards flow again.
A catheter is often inserted into the bladder after the procedure to help drain the urine during the healing process.
Common problems after surgery can include blood in the urine, bladder spasms and cramping.
Sometimes children can suffer from a high temperature or intolerance to liquids after surgery. Children can still be prone to urinary tract infections after a ureteric implant.
Pages in this Section
-
Helen Dolan Clinical Negligence - Joint Head of the Manchester Office 0800 027 2557

-
Lesley Herbertson Clinical Negligence - Partner 0800 027 2557

-
-
Gill Edwards Clinical Negligence - Partner 0800 027 2557

-
Sophie Birch Clinical Negligence - Senior Associate 0800 027 2557

By filling out this form you are authorising Potter Rees Dolan to use the details you provide to contact you regarding your potential claim. Read our Website Privacy Notice.