Uterine Rupture Claims
The expert solicitors at Potter Rees Dolan are here to help you claim compensation if you have suffered a uterine rupture which your assigned medical professionals failed to notice or properly manage.
Uterine ruptures can have a devastating impact on you and your loved ones, and you may have many questions as to what exactly went wrong if this has happened to you. Our professional and caring team of clinical negligence solicitors can help you and your child get the answers you need, as well as a financial award to help you cope with the consequences of the error.
Our clinical negligence team includes leading solicitors Helen Dolan, Lesley Herbertson and Gill Edwards, who all feature in the prestigious Legal 500 and Chambers guides. One of our guiding principles is to personalise our service for every single person we work with and put our clients first.
We want to help, and we’re ready to get you the support and the compensation you deserve. Call our team on 0800 027 2557, or if you’d prefer to send us a message, fill in the contact form on this page, and a member of our clinical negligence team will get back to you.
How can medical negligence exacerbate a uterine rupture?
When a uterine rupture occurs, it should be treated as a medical emergency by the attending medical professionals. You may have been a victim of clinical negligence if one or more of the following applies to you:
- There was a delay in diagnosing and managing the uterine rupture
- Your medical team failed to properly identify existing procedures or conditions that contributed to a uterine rupture
- Medical professionals failed to identify whether a caesarean section was needed when a previous caesarean section had been carried out
- There was a delay in carrying out an emergency caesarean section once a uterine rupture has been diagnosed
What is a uterine rupture?
A uterine rupture is typically where a scar from a previous caesarean section tears open during childbirth. They are fairly uncommon, but can be a risk for mothers who choose to give birth vaginally after having had a caesarean birth in a previous pregnancy.
In exceptional cases, uterine ruptures can occur without a previous caesarean scar - although these cases are extremely rare.
How we can help
Potter Rees Dolan’s clinical negligence team has earned a reputation as one of the very best in the UK. Boasting a combined experience in serious injury law of over 60 years and comprehensive medical insight, the team has an unwavering dedication to helping families recover the compensation they deserve.
Helen Dolan, head of the department, was featured in the Chambers 2019 legal guide, which noted that she “regularly handles complex claims”. The guide highlighted a quote from a client praising “her attention to detail and knowledge of the case, inside and out”.
The same publication said Lesley Herbertson “is very good on the complex details of the case and is able to translate this to clients”.
Meanwhile, Gill Edwards was described as being "incredibly good with clients - they really warm to her", and earned praise from a client, who said: "She is very good on the medical details."
Additionally, our entire clinical negligence department received a recommendation from Chambers 2019, which described them as “a well-regarded team with an impressive caseload of complex clinical negligence work”.
Our clients regularly tell us that it is the empathy and care with which we act that sets us apart. We specialise in serious and catastrophic injuries, so we know how difficult it can be to live with severe disability. It is our aim, therefore, to make the claims process as stress-free for you and your family as we can.
Funding
Many clinical negligence cases are funded on a “no win, no fee” arrangement, also known as a Conditional Fee Agreement. We can investigate your potential claim and you will not have to pay us anything if your case is not successful. In our first meeting, we’ll explain how a Conditional Fee Agreement works.
If you already have a legal expense insurance policy in place, we’ll always start by investigating whether you can use the same policy for your case before we consider whether a Conditional Fee Agreement might be more appropriate.
What happens next?
We will discuss your circumstances in detail and help you understand whether or not you have a case. If you do, we will help you gather all of the evidence needed to build a strong case and give you the best chance of recovering an appropriate amount of compensation.
Your medical records are where we will look first - we will obtain them and study them with you in detail, before instructing independent experts to advise on whether or not you or your family member has received substandard treatment.
Once we have positive expert evidence supporting your claim, we will initiate court proceedings. We always try to progress the claim as quickly as possible, while allowing opportunities to adequately settle the case early.
If it is possible, we work to obtain an interim award. This can have a significant impact on those that have suffered the devastating consequences of uterine ruptures by providing money to cover care costs for your child, as well as compensating for any loss of earnings as you recover from the extent of your injuries.
Contact us today
Please don’t hesitate in calling our team today to get the help and support you need. You can reach us on 0800 027 2557, or request a call back through our dedicated contact page. If you would like to speak to a specific person at the firm, visit their profile on our people page.
FAQs
What are the risks for uterine ruptures?
Potential factors that place mothers at an elevated risk of a uterine rupture include:
- a body mass index of more than 30 at the start of a pregnancy
- having a vaginal birth after a caesarean
- the manner in which a caesarean was carried out in a previous pregnancy
- a past history of uterine surgery
- being induced when trying for a vaginal birth after a caesarean
- blunt or direct trauma to the abdomen
What are the possible complications of uterine ruptures?
Uterine ruptures require immediate treatment, as a failure to act can lead to complications such as:
- organ damage for the mother
- severe blood loss, leading to shock, collapse and injury
- brain damage to the newborn child, including cerebral palsy
- the need for a hysterectomy (removal of the uterus) if the injury cannot be adequately repaired
- the death of the mother and/or child
Useful Information
Emergency Emergency Caesarean Section
This procedure is usually carried out when a normal vaginal delivery would put the mother or the baby at risk.
However, an emergency caesarean is performed when circumstances before or during labour call for an unplanned procedure.
A caesarean section is usually carried out under an epidural or a spinal anaesthetic causing the lower part of the body to be numbed. The procedure usually takes 40-45 minutes but, during an emergency, can be performed quicker.
The risks to the mother in a caesarean section can include an infection of the wound or the womb lining, a blood clot (thrombosis) in the legs or excess bleeding.
Doctors now give the mother a dose of antibiotics before the operation to reduce the likelihood of any infections.
Risks to the baby during a caesarean, according to the NHS, are no greater than a normal vaginal delivery but the most common problem of babies delivered by caesarean is difficulty breathing, although this usually affects babies born prematurely.
Endometriosis
This is a condition where tissue which behaves like the lining of the womb (endometrium) is found outside the womb. This is a common condition which is said to affect around 2 million women in the UK. [source]
The symptoms of endometriosis varies from woman to woman but the most common include; painful or heavy periods, pain in the lower abdomen, pelvis or lower back, pain during and after sex, bleeding between periods and difficulty getting pregnant.
The exact cause of endometriosis is unclear and there are many different theories. One theory is that endometriosis is hereditary where it has been passed down through the genes.
Another theory is that it is caused by retrograde menstruation which is when the womb lining flows backwards through the fallopian tubes into the abdomen instead of leaving the body as a period. The tissue then embeds itself into the pelvic organs and grows.
There is no cure for endometriosis but treatments are available to help ease the symptoms including; pain relief and hormone injections. Alternatively, surgery may be performed to remove the endometriosis tissue through laparoscopy or even hysterectomy.
Endometriosis can sometimes cause fertility problems through damaging the ovaries or fallopian tubes but it is said that up to 70% of women with mild-mid endometriosis have no problems getting pregnant after treatment.
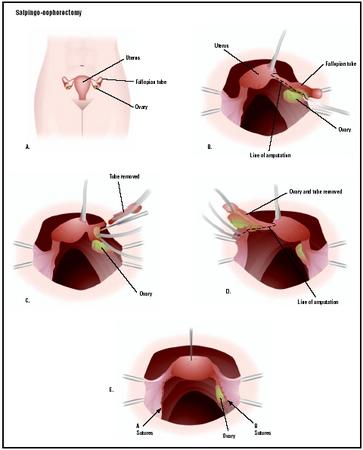
Salpingo-Oophorectomy
This is a surgical procedure which can be either unilateral or bilateral.
Unilateral is where the fallopian tube and an ovary are both removed and a bilateral procedure involves the removal of both sets of fallopian tubes and both ovaries are removed.
The reasons for this surgery to be performed is usually to treat forms of gynaecological cancer or pelvic inflammatory disease.
This procedure may also be done to treat endometriosis as well as if a woman has been diagnosed with an ectopic pregnancy.
Salpingo-oophorectomy is considered major surgery if performed through an abdominal incision and would require three to six weeks to fully recover.
However, if the procedure if performed laparoscopically, the recovery time can be much shorter.
Immediately following the operation, sharply flexing the thighs or the knees should be avoided.
And if the patient suffers with persistent back pain or blood in the urine then it may indicate that a ureterhas been injured during surgery.
Other complications, as with most major surgeries, can include infection, haemorrhage and scars at the incision.
Complications after a salpingo-oophorectomy, however, can include changes in sex drive, hot flashes and other menopausal symptoms if both ovaries are removed.
In general, studies have shown that the complication rate following salpingo-oophorectomy is essentially the same as that following hysterectomy.
Uterine Prolapse
This occurs when the pelvic floor muscles stretch and weaken so there is inadequate support for the uterus, meaning it slips down and protrudes out of the vagina.
Symptoms of a uterine prolapse can include; pain during sex, problems passing urine and the need to urinate more often. However, some women do not have any symptoms.
Childbirth through vaginal delivery can be a cause of a uterine prolapse. The risk of a woman having a prolapse increases as she gets older due to the lack of oestrogen hormone during menopause.
Treatment for a uterine prolapse is not always necessary, however, doctors may advise weight loss to ease stress on pelvic structures and avoiding heavy lifting. Pelvic floor exercises can strengthen the muscles.
If surgery is needed, then a hysterectomy may be performed, whereby the uterus is removed entirely. Or the uterus may be placed back in its original position by re-attaching pelvic ligaments.
Pages in this Section
-
Helen Dolan Clinical Negligence - Joint Head of the Manchester Office 0800 027 2557

-
Lesley Herbertson Clinical Negligence - Partner 0800 027 2557

-
Gill Edwards Clinical Negligence - Partner 0800 027 2557

-
Sophie Birch Clinical Negligence - Senior Associate 0800 027 2557

-
Helen Budge Clinical Negligence - Partner 0800 027 2557

-
Kelly Charlton Clinical Negligence - Senior Associate 0800 027 2557

-
Terri Kelly Clinical Negligence - Solicitor 0800 027 2557

By filling out this form you are authorising Potter Rees Dolan to use the details you provide to contact you regarding your potential claim. Read our Website Privacy Notice.